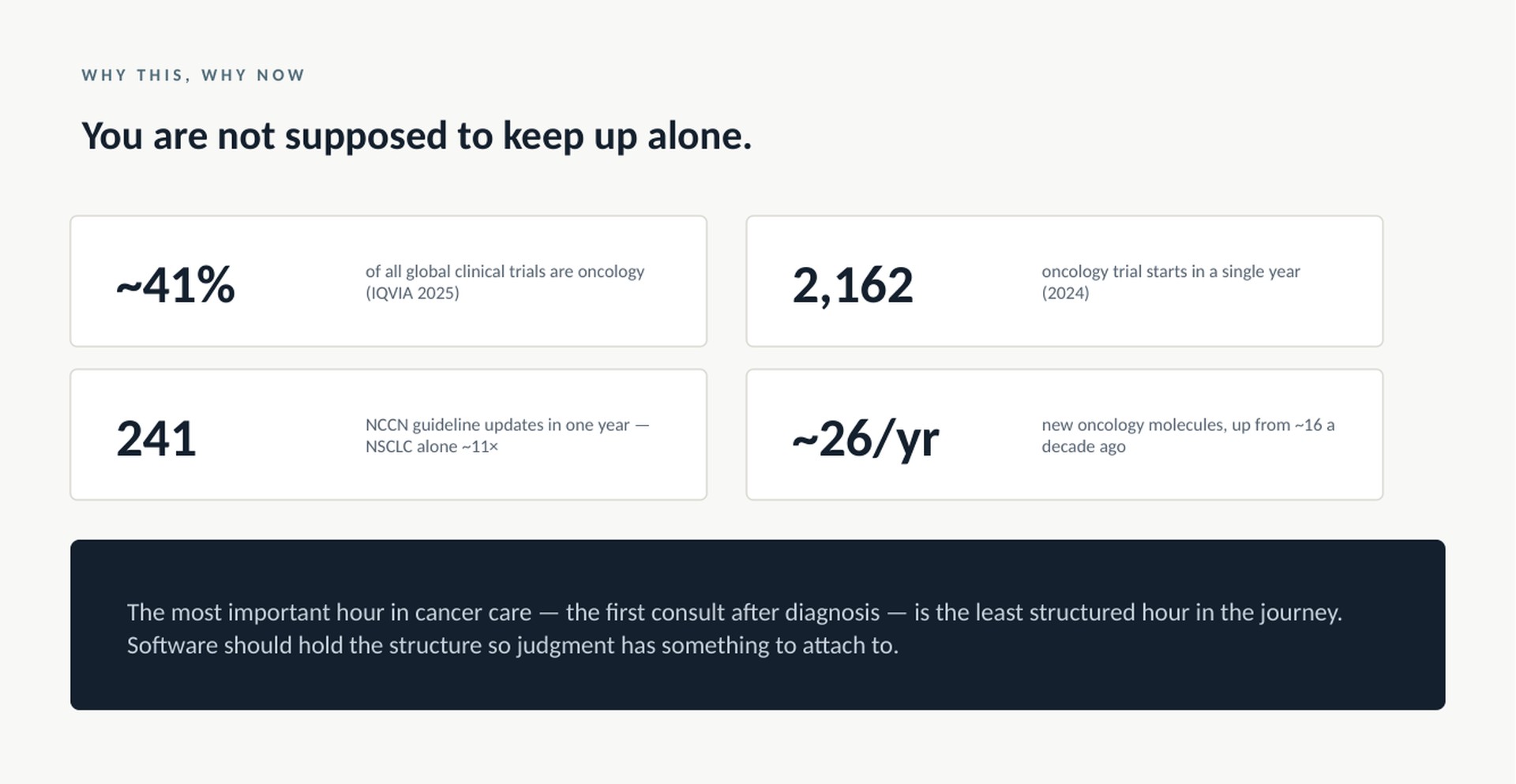
Forty-one percent of all clinical trials running worldwide are in oncology. More than two thousand oncology trials started in a single year. Around twenty-six new cancer medicines reach the market annually now, up from about sixteen a decade ago. The NCCN library — 88 guidelines — was revised 241 times in one year. Non-small cell lung cancer alone was updated eleven times. Nearly once a month, for one disease.
That is not a knowledge base. That is a moving target.
I trained in an era when a good oncologist read the journals, attended the meetings, and carried the field in his head. For most of us, that era is over. There are exceptions — colleagues with an extraordinary command of the literature, and I work with some of them. But watch how even they practise: the WhatsApp group where a difficult case gets argued at midnight, the tumour board, the corridor conversation at a conference. Collective decision-making exists precisely because in modern oncology there is usually more than one defensible answer. And the sharpest command I have seen is always command of a slice — breast, myeloma, thoracic. Depth in a slice is achievable. The breadth, at this velocity, is not.
So the question I keep hearing — can AI be trusted in the clinic? — is the wrong question.
The right question is: which layer do you trust it in?
The problem was never the model. It was the architecture.
When clinical AI first arrived in the consult room, we took a general-purpose chatbot — built to be fluent, not accountable — and dropped it into medicine's most consequential hour. No chart. No audit trail. No ability to decline with a reason. When it stumbled, we blamed the model. But that was never a model problem. It was an architecture problem.
And the deepest flaw in the chatbox is not trust. It is context.
Every chat starts blank. The patient exists in your head, and the machine sees only the fragment you had time to type — a line about the diagnosis, the one lab value you remembered, the question. It answers that fragment, fluently. And whatever you left out — the creatinine, the cardiac history, the line of treatment she already failed — does not weaken the answer. It is simply, silently, not in it. The confidence stays the same.
Now invert it. Put the AI inside a workspace where the whole case already lives — staging, pathology, prior lines, comorbidities, the scanned documents nobody re-reads. The question is no longer the container for the context; the case is. Ask the same question, and the machine reasons over the complete patient — not the remembered one.
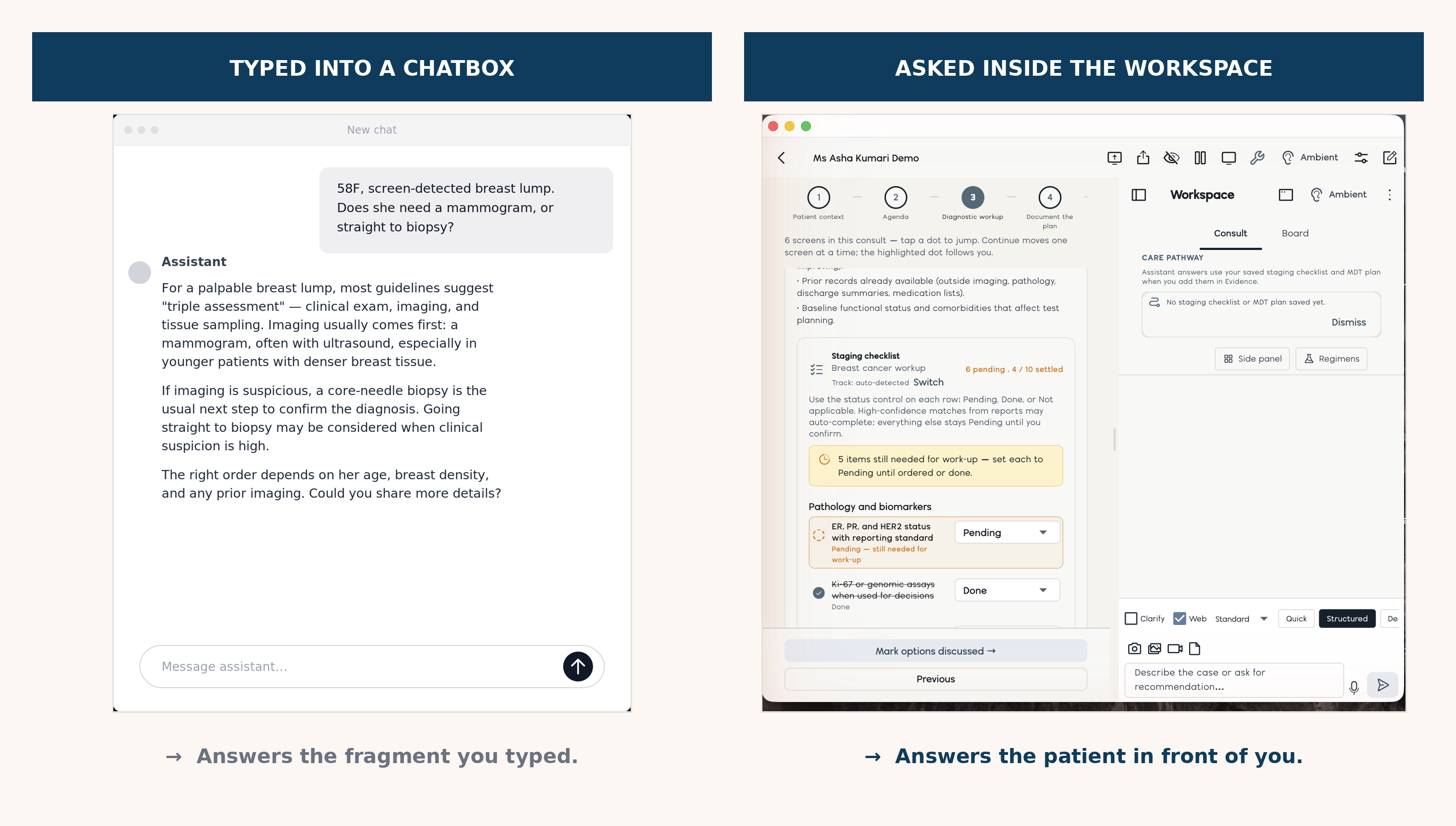
A chatbox answers the question you typed. A workspace answers the patient in front of you.
The honest shape of clinical AI — three layers
That, to me, is the honest shape of clinical AI — three layers, each doing what it is built for.
A deterministic layer for what must never drift: staging math, screening eligibility, hard-stop safety checklists. These are rules, and rules should be code. Code gives the same answer at 9 AM and 9 PM, on the first patient and the fortieth. Code, not conversation.
A guideline-anchored layer for what must be citable. If a system ranks options, each should carry its evidence tier and a pinned citation — and because the guidelines moved 241 times last year, the audit question is not what does the guideline say? but what did it say on the day this decision was made? Guidelines move. Accountability shouldn't.
A generative layer that works inside the full case — reading what no clinician has time to read, retrieving what matters to this patient, synthesising it against evidence that changed since the last time you looked. Go back to the arithmetic at the top of this piece. This is the only realistic answer to it. Not a machine that decides for you — a machine that makes sure the decision you take is made on this year's oncology, with the whole patient on the table.
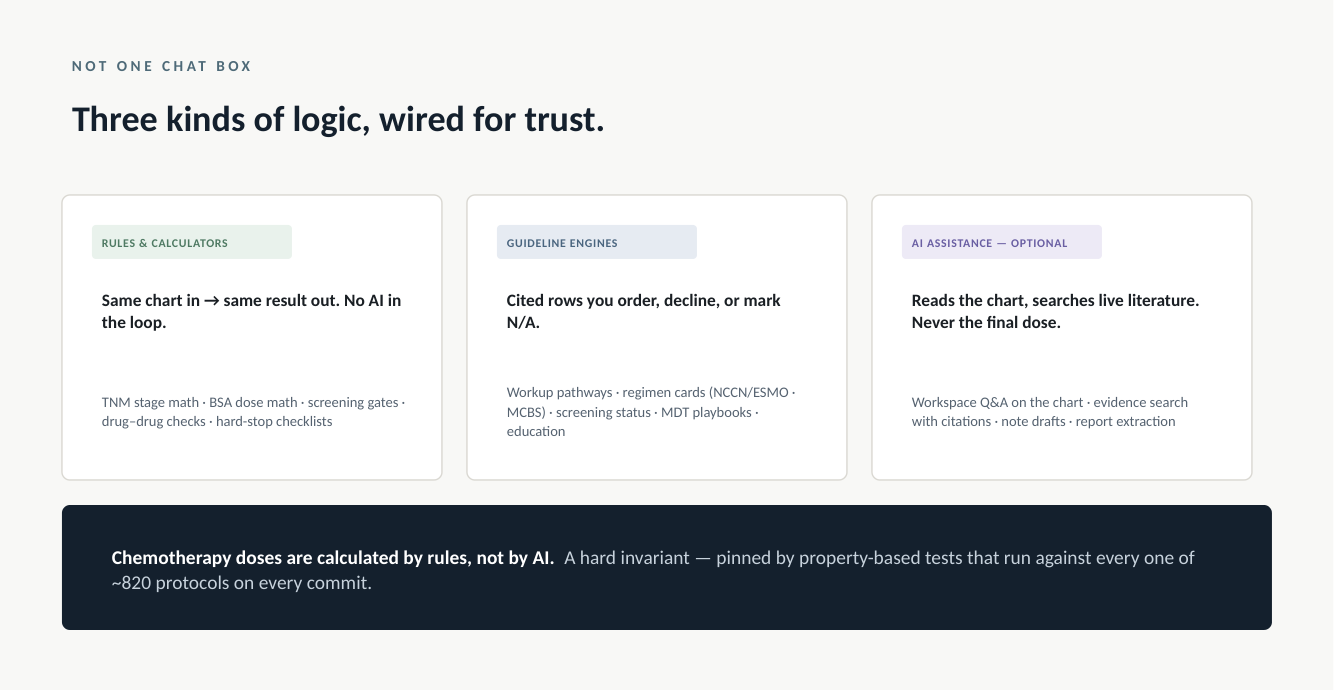
One line should stay non-negotiable wherever these systems go: chemotherapy doses are calculated by rules, not by AI.
What to ask before you trust any of it
For colleagues and hospital teams evaluating clinical AI this year, my checklist has become short. Does it see the whole case, or only the fragment you typed? Does every recommendation carry its citation and its guideline version? Can it decline to answer — with a reason — instead of improvising? And does it make you faster at being current, rather than slower at being safe?
Most of what I have seen fails at least one of these. Not because the models are weak — they are astonishing — but because the architecture around them was designed for demos, not for the fortieth patient on a Tuesday OPD.
The field will get this right eventually. A specialty generating evidence faster than any human can read it was always going to meet machinery that reads faster than humans forget. The open question is whether the systems that win will be built around the consult room as it actually works — or around what a slide deck imagines it to be.